This article, written by Dave Fornell and published by Cardiovascular Business, summarizes how a new application of artificial intelligence (AI) to automatically assess soft coronary plaques in the coronary arteries, presented at the Society of Cardiovascular Computed Tomography (SCCT) 2022 meeting, could change the practice of cardiology by enabling a sort of “mammogram for the heart” type serial screening in the years to come.
Numerous session speakers detailed how soft plaque characterization and accurate quantification could be used as a baseline, followed by future serial, noninvasive CT angiograms (CTA). Similar to mammography, new exams could be compared to priors to assess progression of disease and the need for more aggressive drug therapy or lifestyle changes. This data could potentially be used as a justification for high-cost drugs to lower cholesterol in select patients. Serial CT scans showing detailed plaque information can also show regression of plaques due to effective medical therapy and lifestyle changes.
“Soft plaque evaluation is something we have been talking about for nearly two decades, but the limitations always have been how to overcome the large amount of post-processing time,” explained SCCT President Eric Williamson, MD, MSCCT, associate chair for radiology informatics at Mayo Clinic Rochester, supervisor of the radiology artificial intelligence program and professor of radiology at Mayo Clinic. “Previously, it was very time and labor-intensive. But, with the advent of AI and machine learning, this process can be automated.”
For more than a decade, CT systems and advanced visualization software vendors have offered tools to assess soft plaque, but it only showed plaque listed by various Hounsfield units (HU) densities and did not offer a definitive description of what this meant. To quantify the plaque, radiologists or cardiologists had to decide what these units meant and then contour each part of the plaques in the vessel segments by manually drawing lines around these areas, calculating the area they occupied, and then adding all these numbers up. Williamson said it was not feasible for physicians to spend time doing that, so imagers generally just offer a broad overview language to eyeball an assessment of the plaques. Williamson said the AI removed a large amount of time and variability between image readers, and allows for reproducible analysis.
He said at least four vendors showed new plaque assessment technologies at SCCT this year, and two of them now have U.S. Food and Drug Administration (FDA) clearance. These advances led to several sessions at this year’s meeting on the importance and evaluation of soft plaque. Several speakers said this technology will likely be the way of the future and move cardiology toward the long-sought goal of preventive care, rather than reactionary care to advanced disease and acute coronary events.
“We have developed a lot of new technologies that are driving down CT radiation dose levels, and we are getting to the point where we could certainly do a coronary CT angiography — maybe not quite at mammogram doses — but close,” Williamson said. “When you think about the success of our cancer screening programs, as we start to think about our risk and benefits, coronary atherosclerosis kills a lot more people than these other diseases.”
Creating a cardiac screening program similar to several cancer screening programs now in use could enable much earlier preventive care, long before it develops into a symptomatic disease. While cancer is the focus of current imaging screening programs for breast cancer, lung cancer and colon cancer, cardiovascular disease is actually the largest cause of death in the world. Cardiovascular disease kills close to 700,000 Americans per year, while cancer deaths are just over 600,000, according to Centers for Disease Control and Prevention (CDC) statistics.[1]

One of several pages of an artificial intelligence report on the coronary plaque from a patient’s CTA scan. The FDA-cleared software developed Cleerly enables rapid soft plaque AI assessment, overcoming the previously tedious and time consuming manual task of making these calculations. These types of reports may enable a new level of preventive care in cardiology, treating patients long before they have symptomatic disease.
AI can overcome the complexity and time involved in evaluating coronary artery plaques
Several coronary CT angiography (CCTA) experts echoed the need for AI to perform the complex and time-consuming task of soft plaque assessment.
“Soft plaque composition is quite complex and the whole process of evaluating these plaques is becoming complex for imagers as well, and that is where the AI comes in,” explained former European Society of Cardiology (ESC) President Prof. Jeroen Bax, director of noninvasive imaging and director of the echo laboratory, Department of Cardiology at the Leiden University Medical Center in The Netherlands. “Looking at the products from these vendors, it becomes clear that visual analysis on the plaques is not enough. We need need to have a better understanding of the composition on the plaques and the only way to do that is through quantification. It will become important that we can assess the extent of the non-calcified lesion.”
Automated plaque analysis can quantify the amount of plaque and the specific kinds of soft plaque much faster and more accurately than a human. This may enable better patient care and earlier interventions.
“This is a really exciting area right now, where we can use AI to process the CT images and pull in a new wealth in data,” said Ron Blankstein, MD, SCCT, associate director, cardiovascular ima-nag program, director of cardiac CT, and professor of medicine, Harvard Medical School, Brigham and Woman’s Hospital. “This is something that today takes a long time to do manually, which is why nobody really uses this in clinical care. But this is going to be the future, where with every coronary CTA, we will be able to provide a very detailed report about how much plaque someone has. Ultimately, this will tell us the amount of risk a patient has and the amount of benefit a patient might get from preventive therapies.”
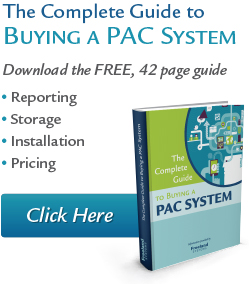
Examples of Caristo’s fat attenuation index (FAI) CT imaging of coronary vessel fat to show inflammation.
Analyzing coronary inflammation using CT fat attenuation index (FAI) imaging
Beyond soft plaques, Blankstein was also excited about a new AI technology from Caristo at SCCT, which uses an algorithm to analyze CTA scans for the tiny layers of fat surrounding coronary arteries. Using a scale of fat attenuation index (FAI) on the CT scan, the technology visualizes inflammation of the vessel wall. This can confirm if a soft plaque is inflamed, which can accelerate plaque progression and rupture. This technology was cited as one of the most exciting new advances discussed at both the 2020 and 2021 virtual SCCT meetings.
“We can see inflammation in the vessel wall, so this may allow us to look at risk assessments even before a patient develops plaque,” Blankstein said. “Or, this can be used to tell us if a patient does have plaque, if it is stable, or do they have a significant amount of ongoing inflammation, where we expect a faster plaque progression.”
FDA-cleared AI technology to assess soft coronary plaques
Two companies currently have FDA for AI coronary soft plaque assessments — Cleerly and Elucid.
Cleerly maintains its plaque assessment goes beyond traditional measures of heart disease, with a comprehensive assessment of each coronary artery and branch. The AI identifies, characterizes, and quantifies plaque buildup in each vessel to generate a comprehensive report. The company says this data can help determine a patient’s risk of a heart attack and develop a treatment plan. Speakers on this technology at SCCT said it could be leveraged for personalized medicine rather than the usual one-size fits all approach in cardiovascular disease prevention.
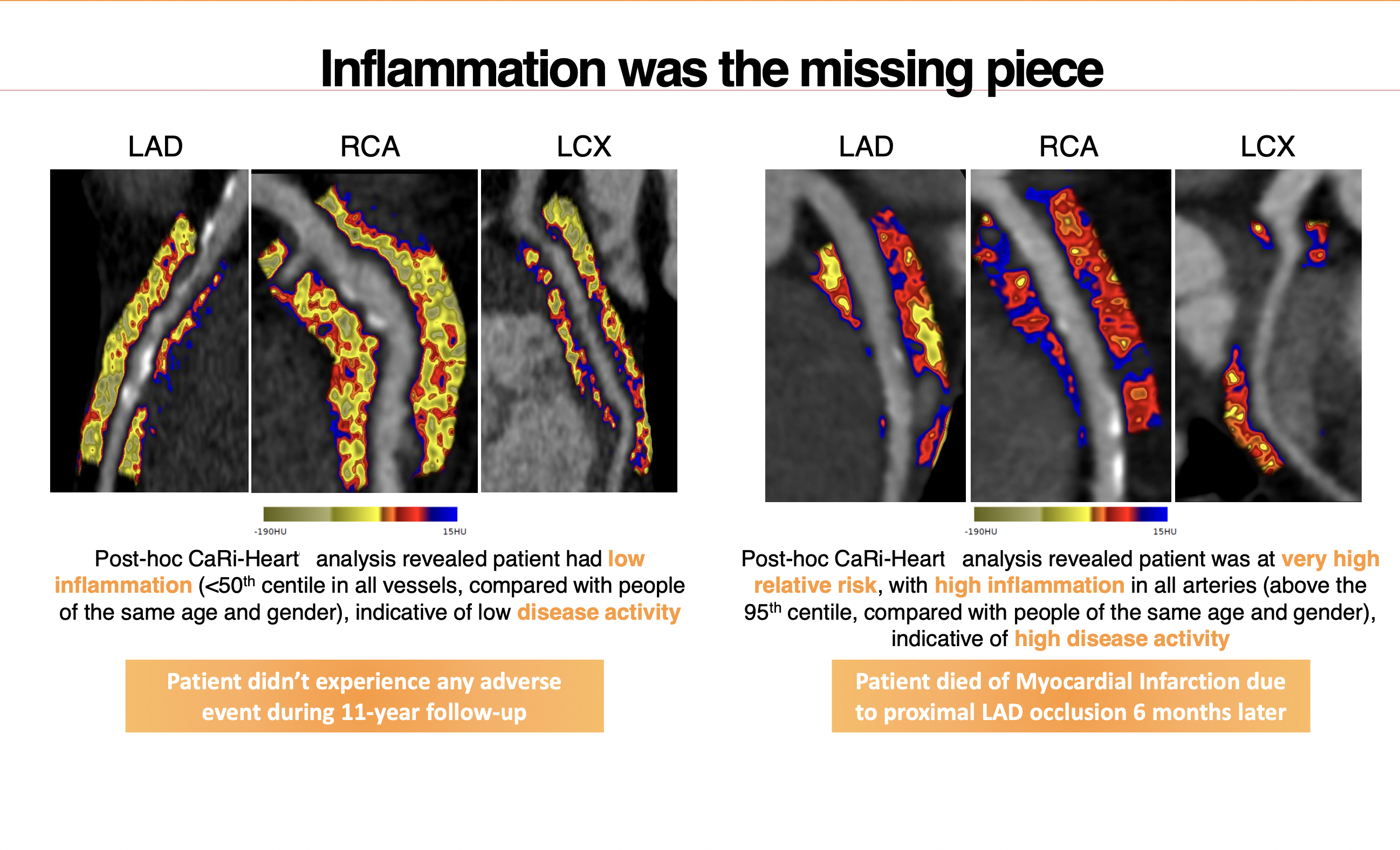
Cleerly includes an automated coronary tree model made from the scan that color codes area of different types of plaques and flags areas of interest for the radiologist or cardiologist. It also auto segments and reformats the coronary vessels to show the plaque on the CT MIP images. A detailed report offers a list of automated quantifications.
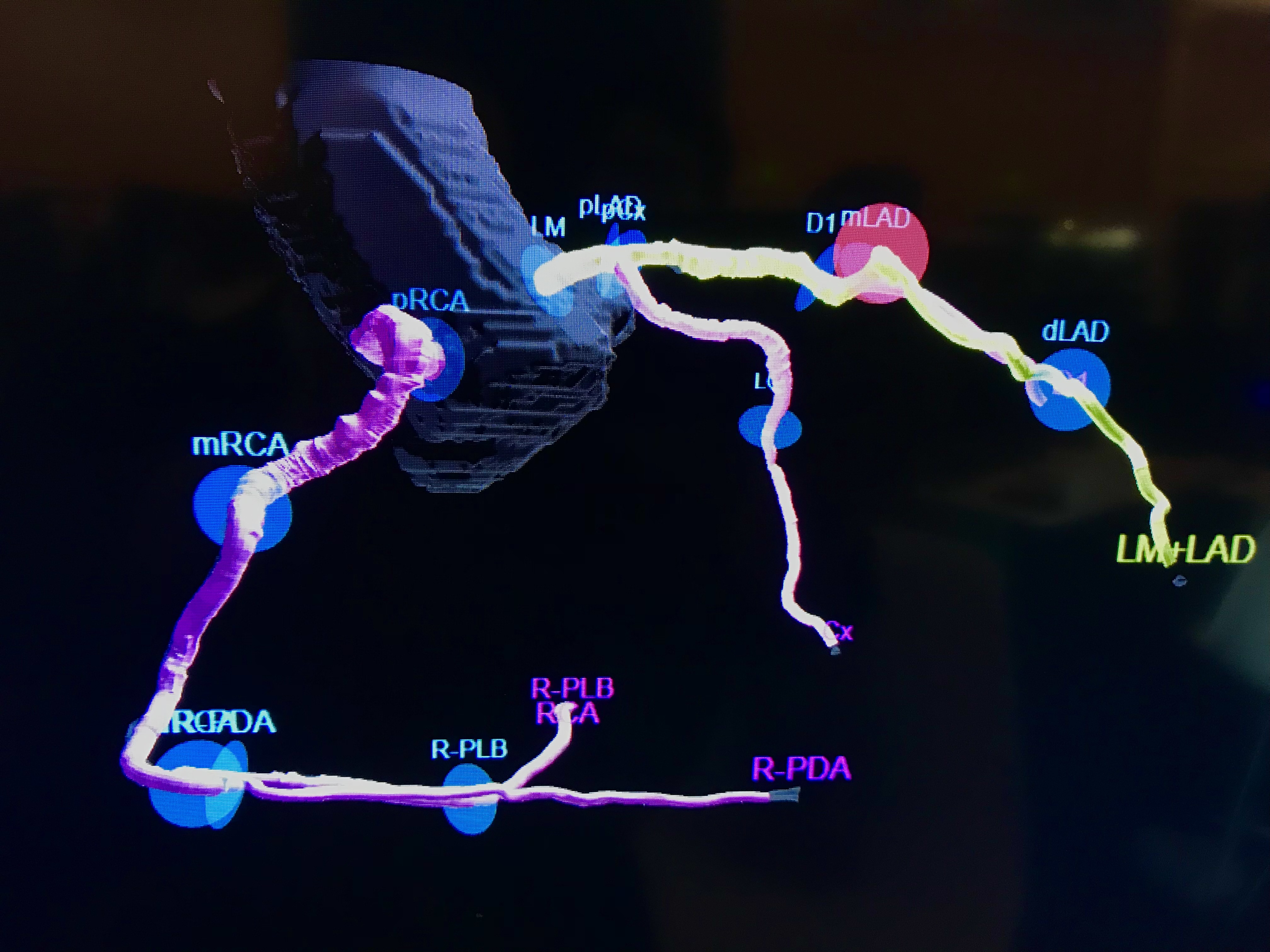
Elucid’s technology analyzes CT angiography using AI computer algorithms that were developed using expert histologic examination of thousands of tissue samples. It can objectively quantify the extent and stability of arterial plaque to develop a tailored patient care plan. The system color codes the various types of plaque inside a vessel for easier interpretation of the image and to pinpoint high-risk lesions.
The company said the new 2021 Chest Pain Evaluation Guidelines[2] will increase the number of cardiac CT exams where this technology will be able to offer additional information of the patient’s disease and risk factors for future events.
AI-generated coronary tree from a patient’s CT scan showing a color code of areas of interest for plaque burden from the Cleerly software shown at SCCT 2022.
Two key CTA thought leaders left clinical practice to help new plaque AI startups
The two vendors that recently gained FDA clearance for their AI plaque assessment software have been taken more seriously, because two key cardiac CTA experts, both former presidents of the SCCT, left or will soon be leaving their academic and clinical posts to work for these companies full time.
CTA pioneer James Min, MD, said he saw a large opportunity in the technology to advance cardiology. He felt strongly enough to leave his job last year as professor of radiology and medicine at Weill Cornell Medical College and the director of the Dalio Institute of Cardiovascular Imaging at NewYork-Presbyterian. He is now the founder and CEO of Cleerly.
Min said the development, validation, and dissemination of Cleerly’s technology offers him an opportunity to translate the large-scale clinical trial research he has worked on over the last 17 years into daily clinical practice. He said this type of innovative solution for coronary heart disease has not existed in the marketplace to date.
Fellow past SCCT President Todd Villines, MD, also announced in a session at SCCT 2022 that he is soon leaving his post as an endowed professor and clinical researcher at the University of Virgina to take over as chief medical officer of Elucid.
“Our current paradigm relies too much on atherosclerotic symptoms and ischemia,” explained Villines. He said cardiology largely bases patient care on these factors rather than looking at the root cause of the disease with the soft plaques. Villines said “our future paradigm” will be AI-based plaque assessments to enable much earlier detection of disease.
Example of the CT image, AI plaque assessment, cross section of a coronary plaque AI assessment and the matching histology for comparison from the same vessel segment from testing of the Elucid AI soft plaque analysis software.
Taking coronary risk assessments beyond calcium scoring to wider cardiovascular disease prevention
CT calcium scoring (CAC) is a common imaging exam that assesses a patient’s risk of further coronary events by looking at the amount of calcium in the coronary vessels. Today, calcium scoring is largely automated by AI and it is considered a primary cardiac risk assessment and is recommended in the 2018 Guideline on the Management of Blood Cholesterol.[3] However, Bax said calcium is formed when a plaque ruptures and the vessel repairs itself, so it shows past history. Soft plaque analysis can show the future, and help track the regression of plaque due to drug therapy, he explained.
“Through retrospective analysis where we did a CT and later the patient got an event, we linked back that event to soft plaque on the CT. We noticed that in most patients who had a coronary event, most of the culprit plaques were not calcified lesions. That is what put us in the direction that noncalcified lesions are the ones that are dangerous,” Bax explained. “These are the ones that develop into vulnerable plaques that rupture and cause myocardial infarction. That was a breakthrough when we realized that.”
However, the plaque makeup can be very complex with different components and not all soft plaques are dangerous or will rupture, Bax added. He said more data was needed to understand the variations in plaque makeup to figure out which patients were high risk or not. Today much more is known about the progression of plaque and the role of inflammation. With the new AI assessments, he said cardiology may be able to go in a new direction.
He said this also comes at a time when cardiac CT has drastically reduced radiation dose for the exams over the past decade through new techniques and better detector technology and image reconstruction software.
“The dose of cardiac CT has gone down so significantly, it has become possible for us to treat patients with medications, perform a CT scan and do the AI quantifications with serial exams over time to see what the influence of our treatment is.”
Bax believes the potential for CTA screening and follow-up serial exams with AI assessment offers a tool to help cardiology finally reach a long-sought goal of completely preventing coronary disease in patients and possibly even eventual eradication of the disease over time.